Medical management represents a comprehensive approach to coordinating clinical care, operational efficiency, and financial performance within healthcare organizations. This multifaceted discipline encompasses everything from treatment protocol development to resource allocation, ensuring that providers deliver high-quality care while maintaining financial sustainability. As healthcare becomes increasingly complex, understanding the core principles of medical management has become essential for practices seeking to thrive in a value-based care environment.
Understanding the Core Components of Medical Management
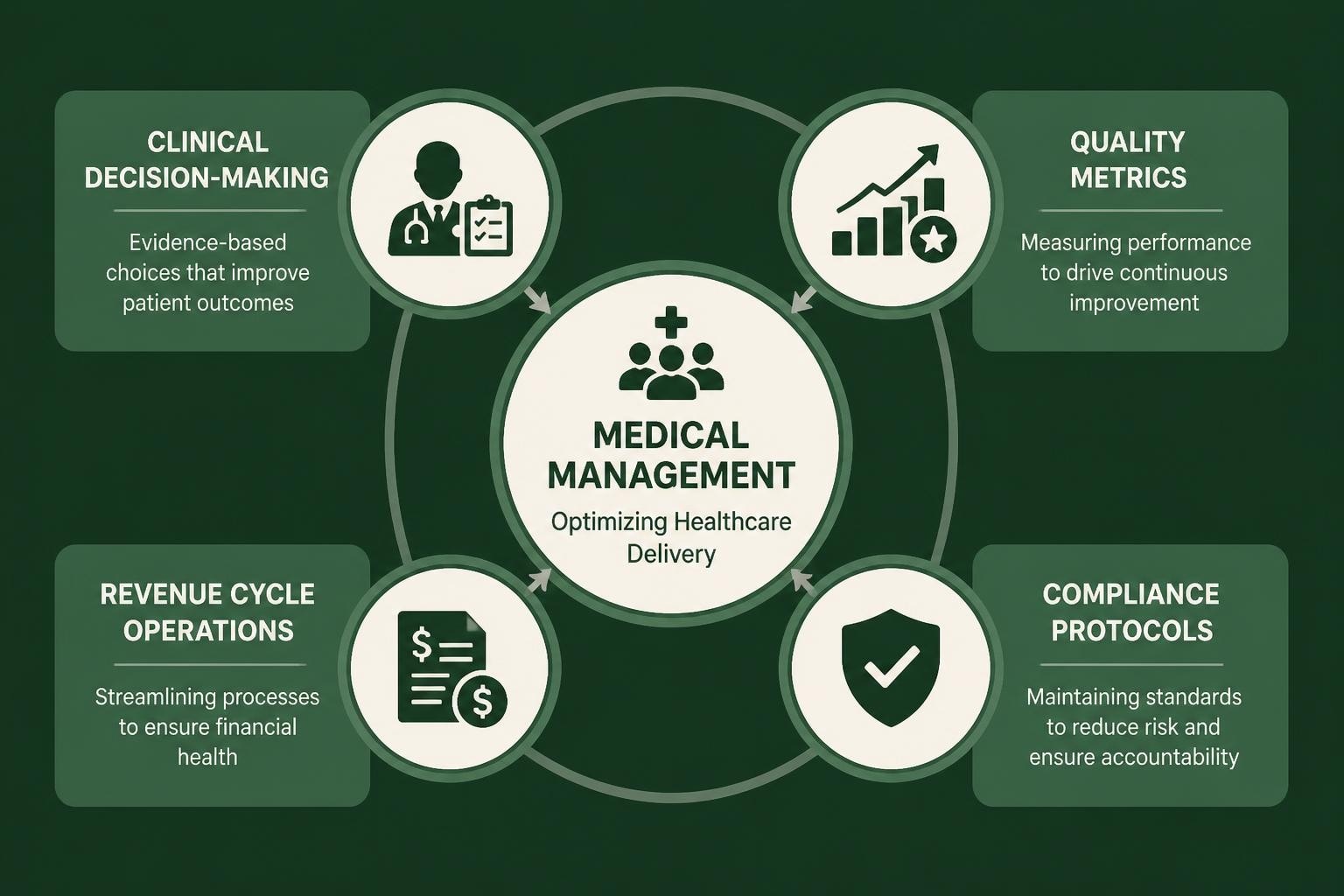
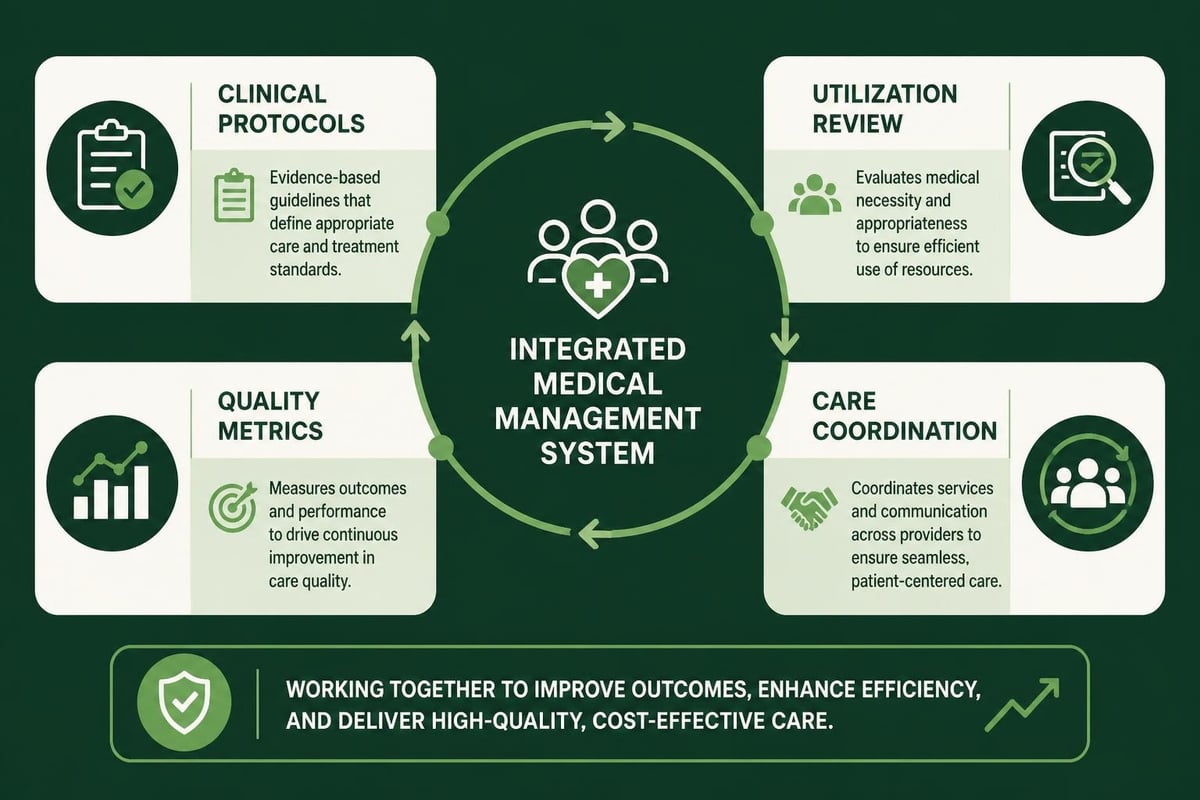
Medical management extends far beyond simple patient care coordination. It involves strategic oversight of clinical protocols, utilization review, case management, and quality improvement initiatives that collectively shape how healthcare organizations function.
Key elements include:
- Evidence-based clinical guidelines and treatment pathways
- Utilization management and prior authorization processes
- Quality measurement and performance tracking
- Care coordination across multiple providers and settings
- Population health management strategies
The appropriate use of medical resources plays a critical role in ensuring that patients receive necessary care without overutilization. This balance directly impacts both clinical outcomes and revenue cycle performance, making it a priority for healthcare administrators.
The Clinical Decision-Making Framework
Effective medical management relies on structured clinical decision-making that combines provider expertise with standardized guidelines. Evidence-based care guidelines provide the foundation for consistent, high-quality treatment decisions across patient populations.
Healthcare providers must balance individual patient needs with established protocols while documenting decisions thoroughly for compliance and reimbursement purposes. This documentation becomes critical when claims undergo review, as payers increasingly require justification for treatment approaches.
Implementing Quality Measures in Medical Management
Quality metrics serve as the backbone of successful medical management programs. These measurements track clinical outcomes, patient satisfaction, operational efficiency, and financial performance.
| Quality Dimension | Key Metrics | Impact on Revenue |
|---|---|---|
| Clinical Outcomes | Readmission rates, complication rates | Reduced penalties, improved reimbursement |
| Patient Experience | Satisfaction scores, access to care | Higher patient retention, referrals |
| Operational Efficiency | Wait times, resource utilization | Lower costs, increased capacity |
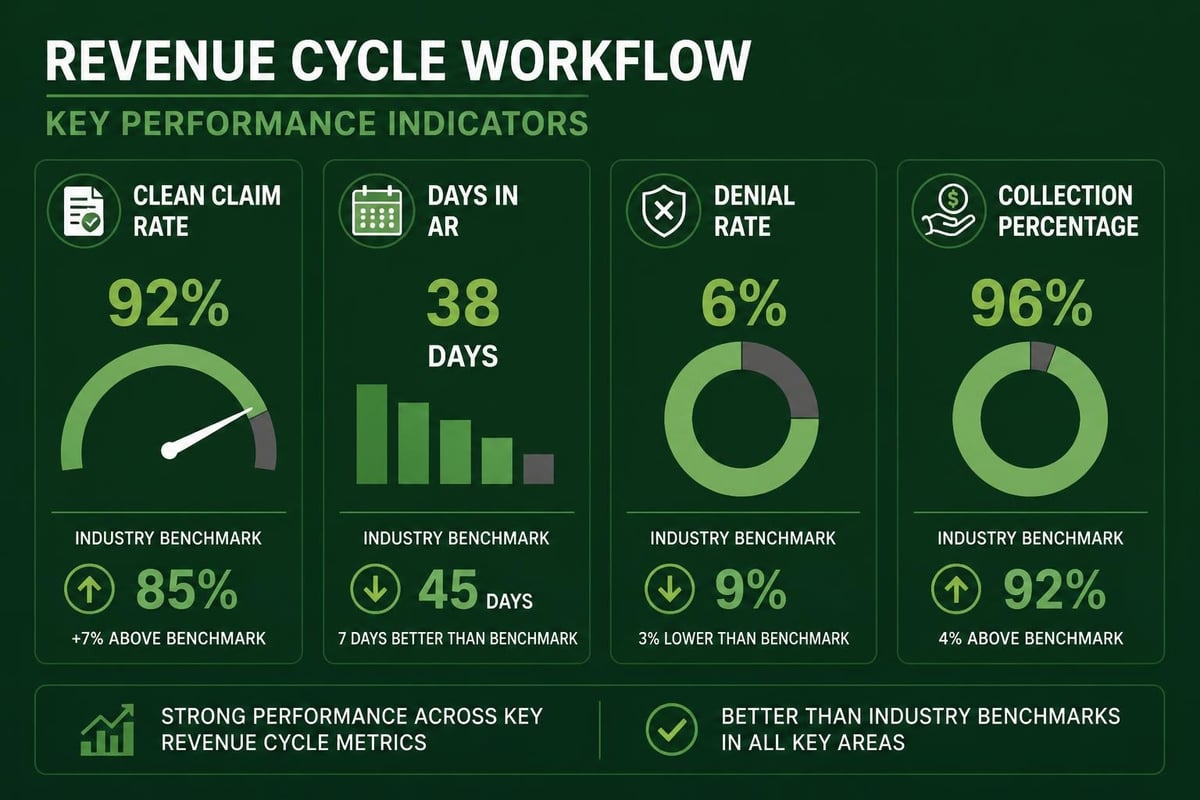
| Financial Performance | Clean claim rate, days in A/R | Faster payments, reduced denials |
The American Academy of Family Physicians emphasizes quality measures as essential tools for improving patient outcomes while demonstrating value to payers. These metrics increasingly influence reimbursement rates under value-based payment models.
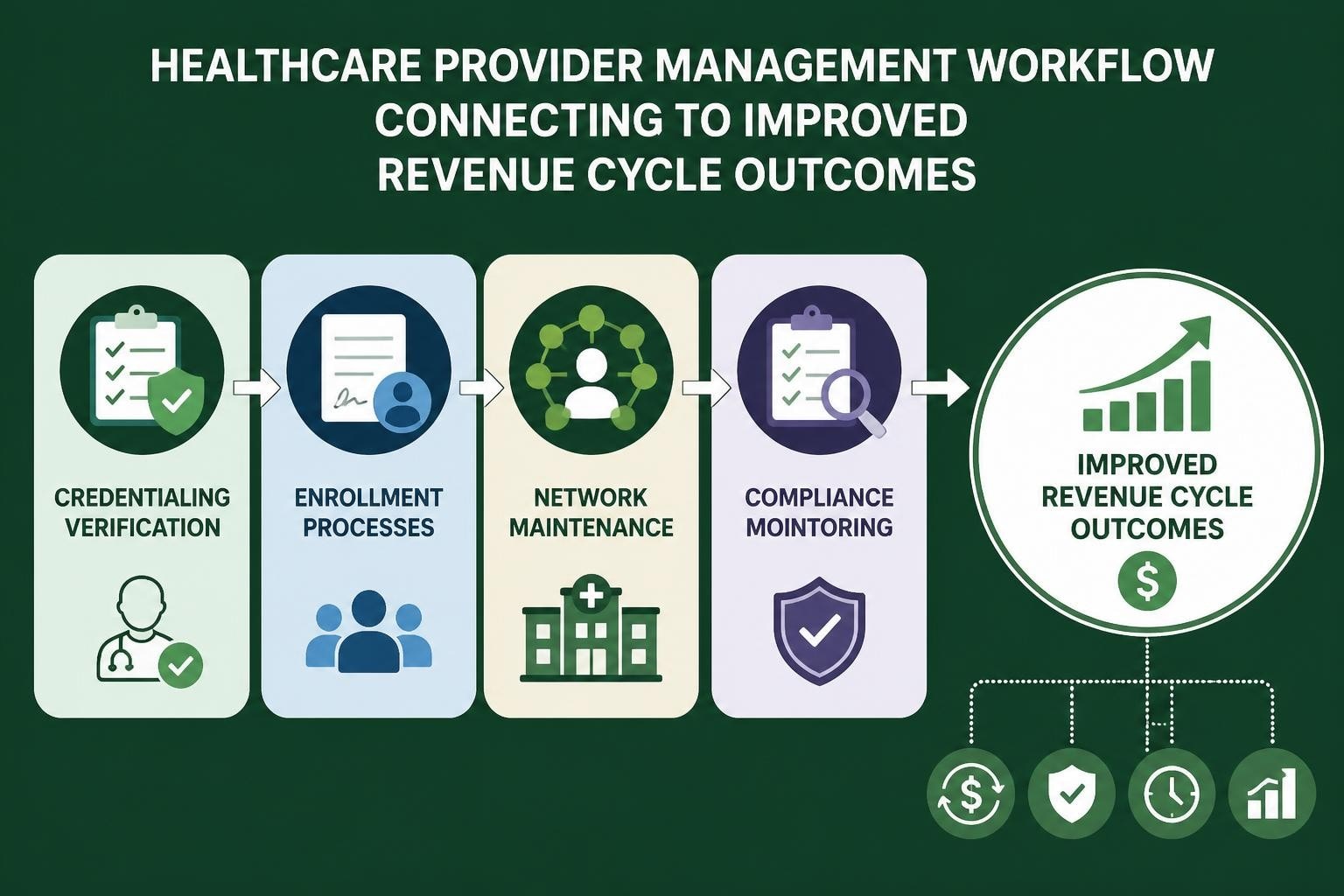
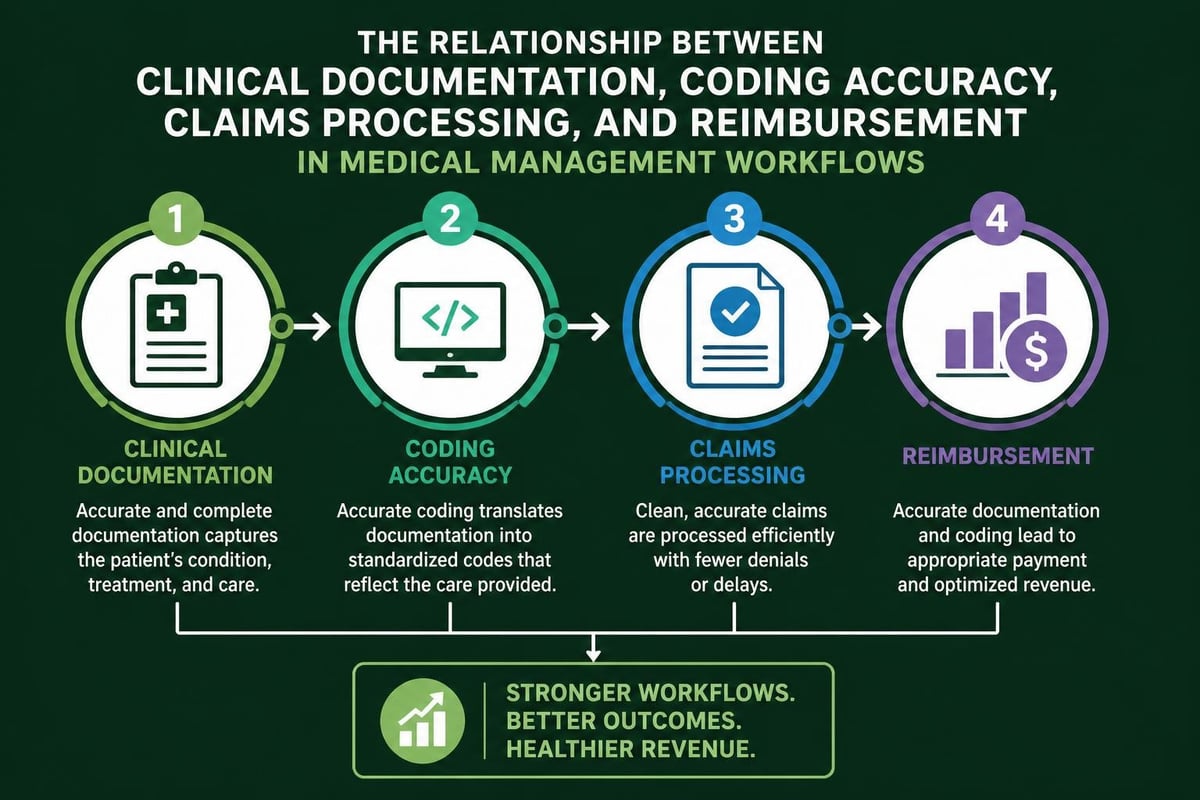
Connecting Medical Management to Revenue Cycle Success
Medical management directly influences revenue cycle performance through multiple channels. Proper utilization review prevents denials related to medical necessity, while thorough documentation supports appropriate coding and billing.
When clinical teams follow established protocols and document care comprehensively, denial management services become more effective at recovering revenues and preventing future claim rejections. The connection between clinical quality and financial performance has never been stronger.
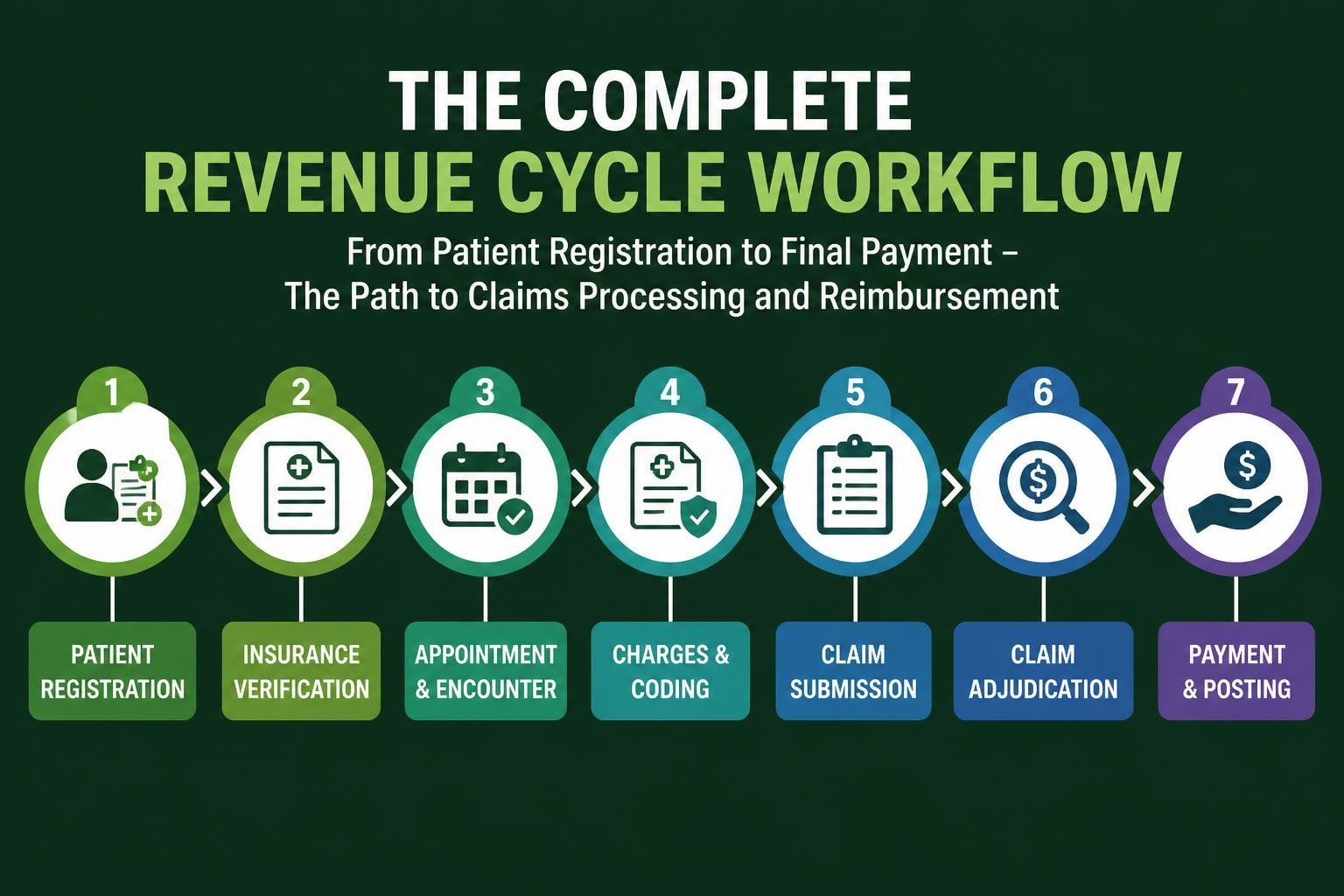
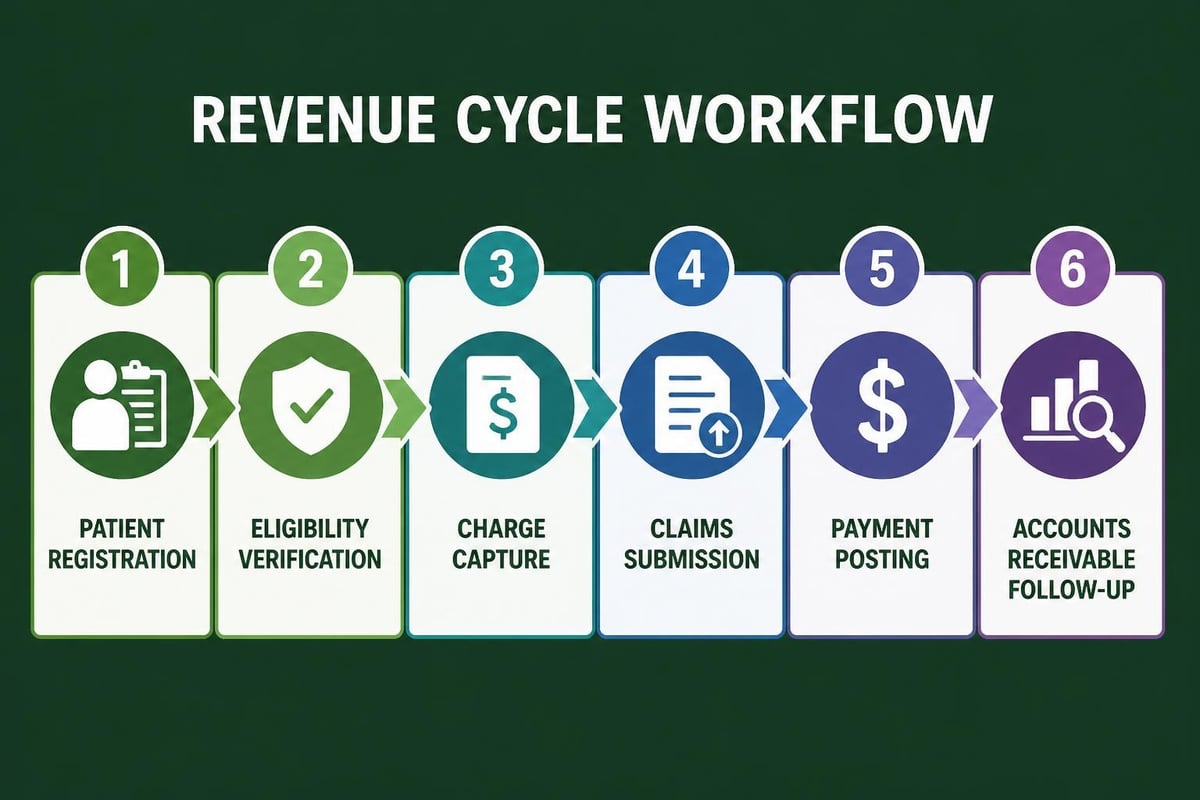
Revenue cycle touchpoints include:
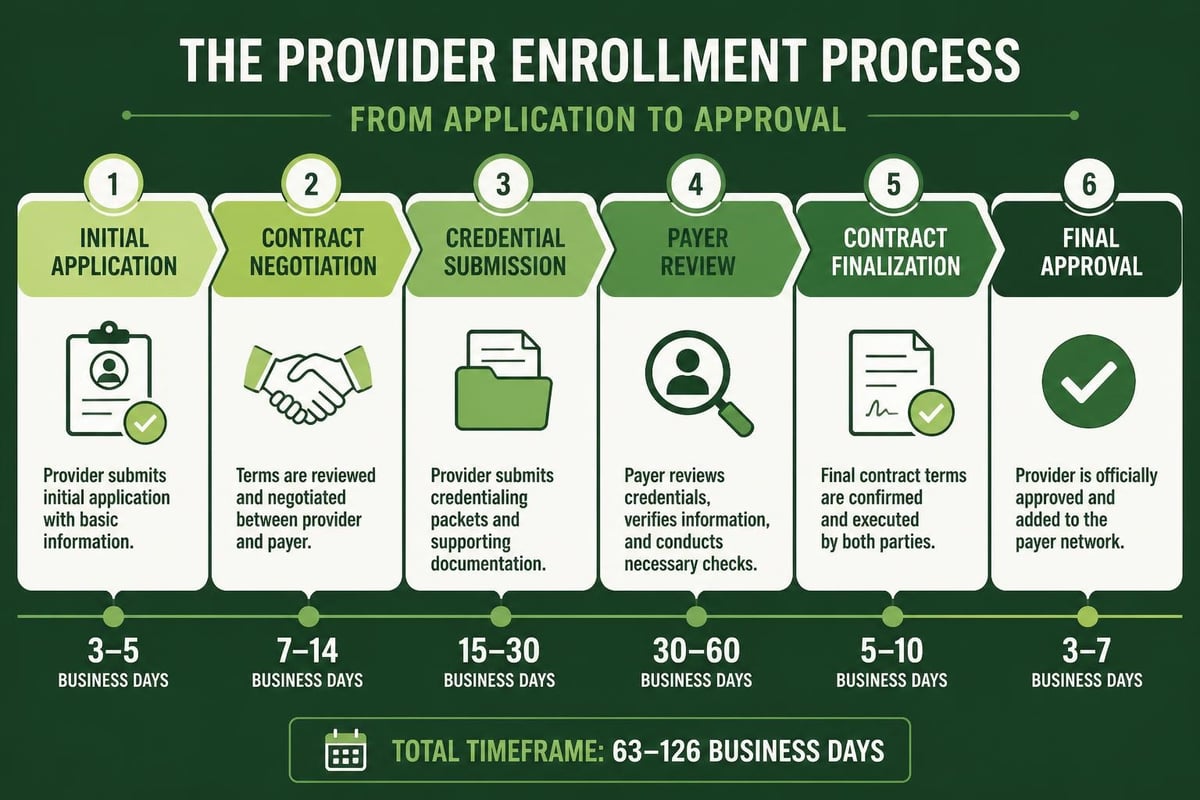
- Pre-service planning – Eligibility verification and prior authorization
- Point-of-service documentation – Real-time coding accuracy
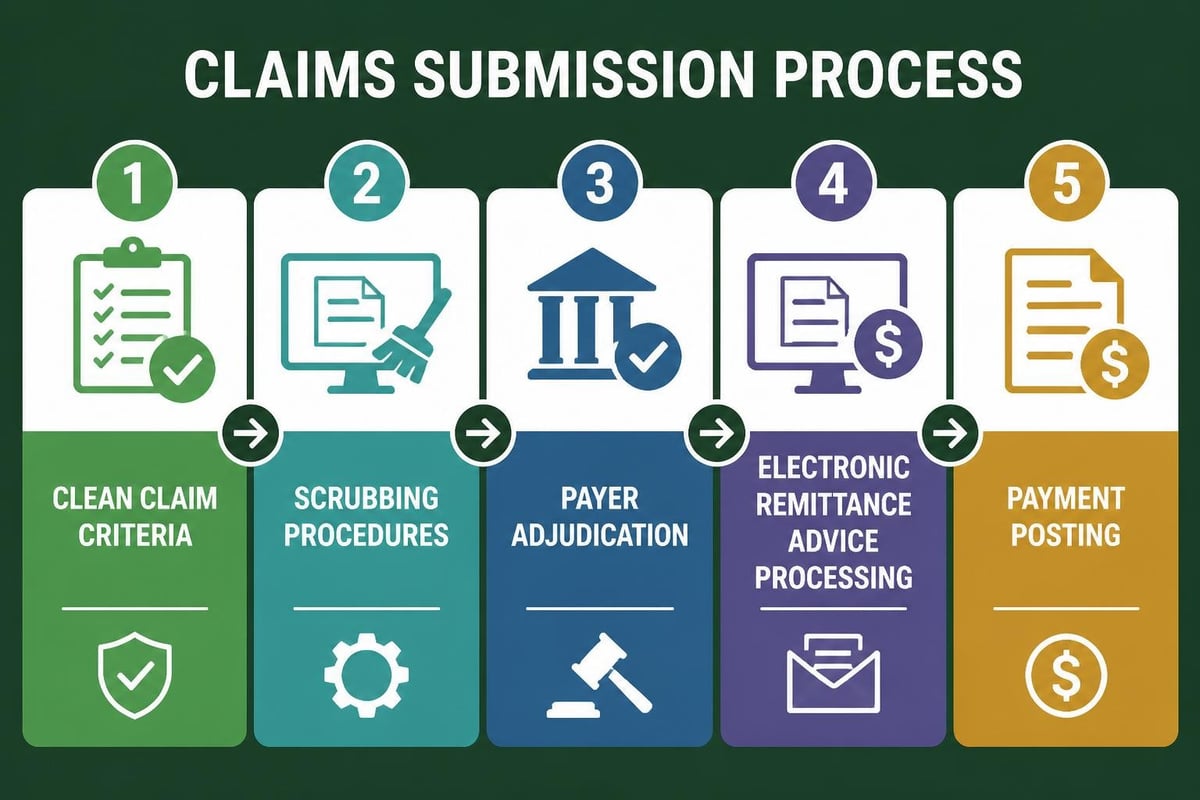
- Post-service review – Claim submission and follow-up
- Ongoing monitoring – Pattern analysis and process improvement
Best Practices for Medical Office Operations
Implementing effective medical management requires structured operational practices that support both clinical and administrative functions. Managing a successful medical office demands attention to leadership, organizational structure, and patient-centered processes.
Streamlining Administrative Workflows
Administrative efficiency directly supports clinical quality and financial performance. When practices optimize their workflows, providers spend less time on paperwork and more time delivering care.
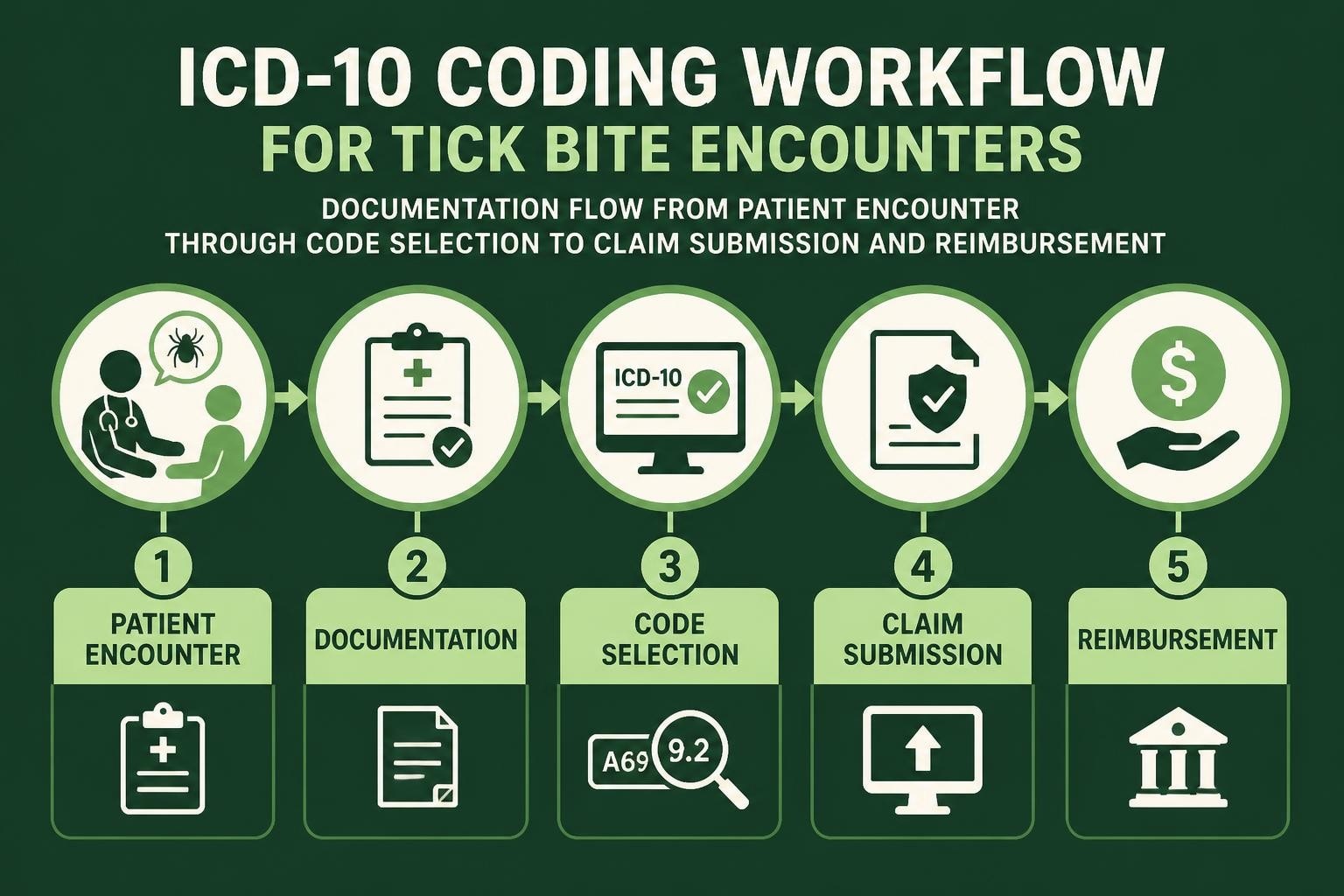
Modern medical billing services integrate seamlessly with clinical operations, ensuring that documentation flows smoothly from patient encounter to claim submission. This integration reduces errors, accelerates payment cycles, and improves overall practice performance.
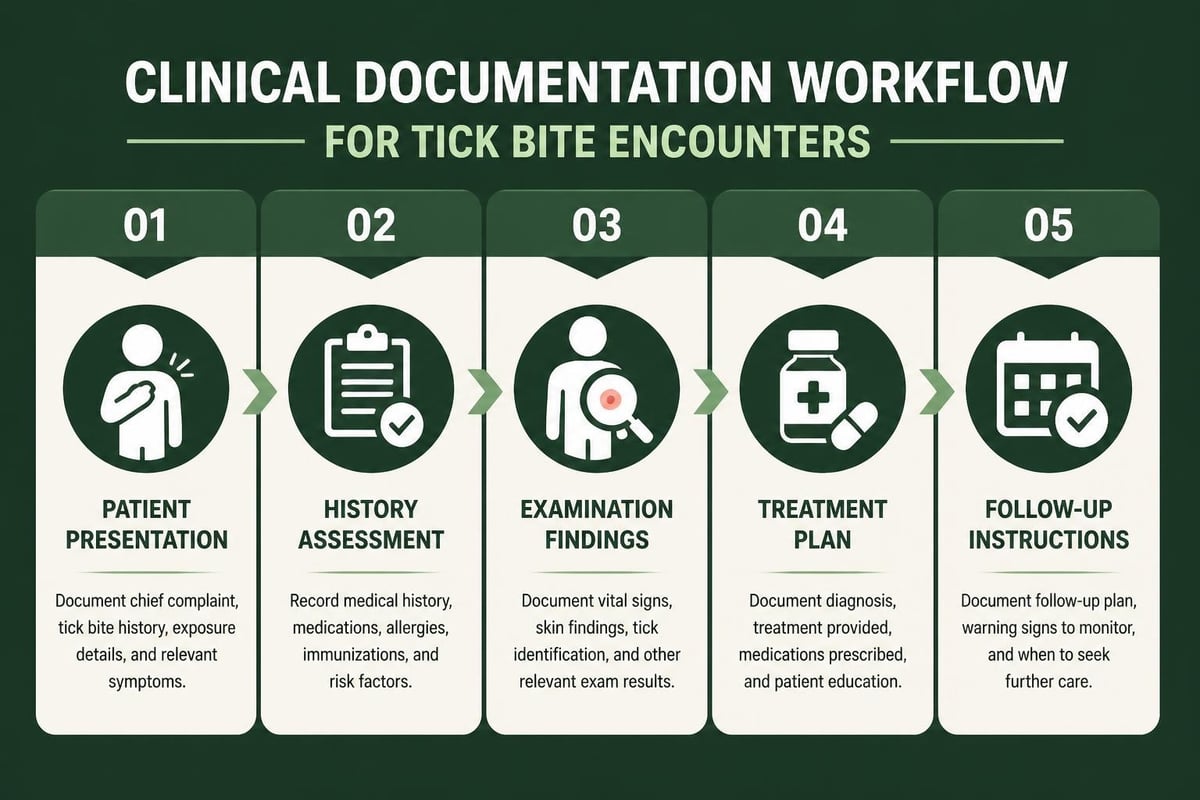
- Standardized documentation templates
- Automated eligibility verification processes
- Real-time coding assistance
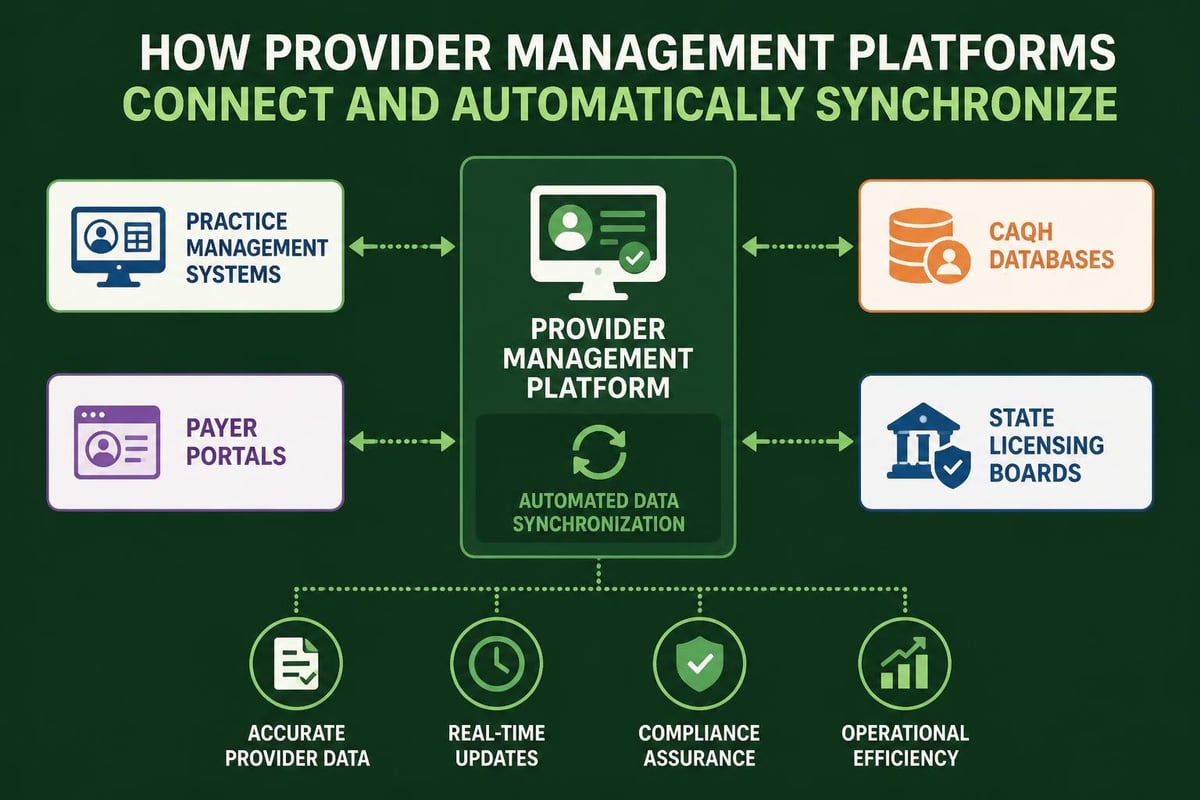
- Integrated practice management systems
- Regular staff training and competency assessment
Technology Integration in Medical Management
Healthcare technology platforms enable sophisticated medical management capabilities that were impossible just a few years ago. Analytics tools track quality metrics, identify utilization patterns, and flag potential compliance issues before they become problems.
Healthcare revenue cycle analytics provide actionable insights that inform both clinical and operational decisions. These data-driven approaches help practices identify improvement opportunities and measure the impact of medical management initiatives.
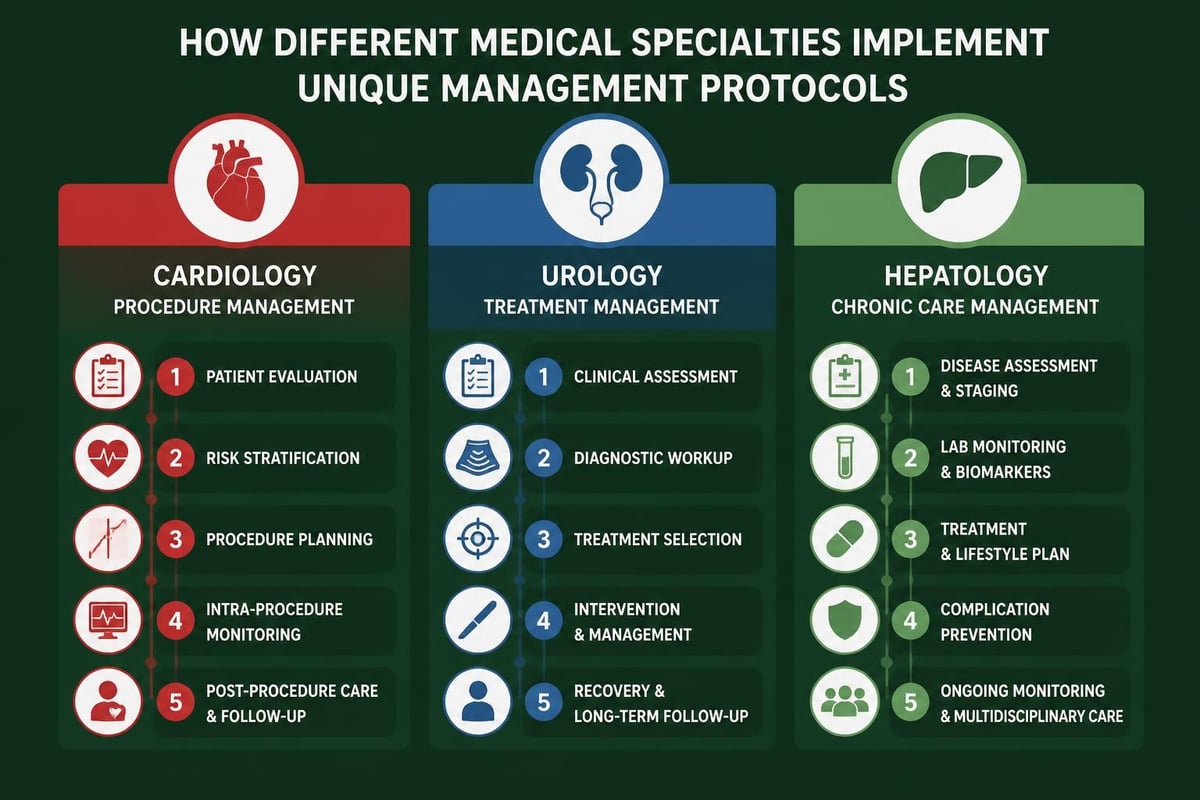
Specialty-Specific Medical Management Considerations
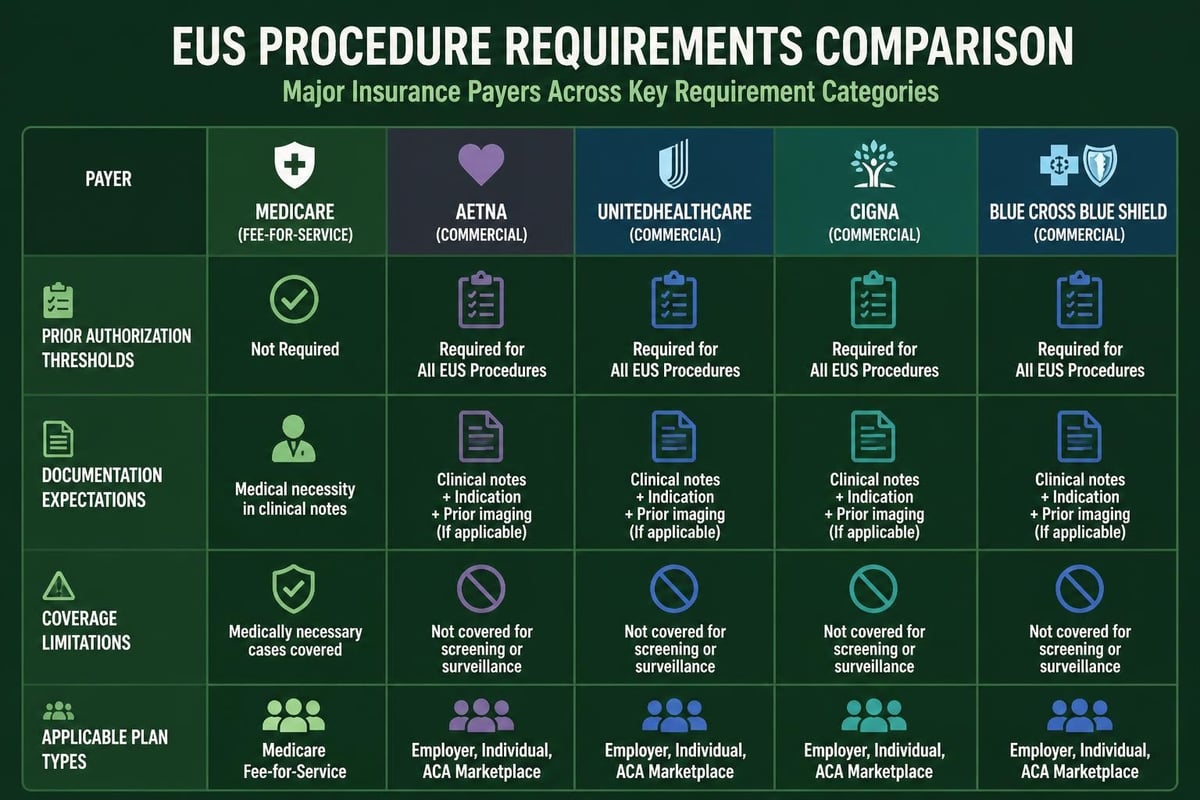
Different medical specialties face unique medical management challenges that require tailored approaches. Gastroenterology practices, for example, must navigate specific protocols like the medical management of microscopic colitis, which requires detailed understanding of treatment algorithms and documentation requirements.
| Specialty | Management Focus | Revenue Impact |
|---|---|---|
| Cardiology | Procedure appropriateness, device tracking | High-value claims, complex coding |
| Urology | Utilization management, bundled payments | Episode-based reimbursement |
| Hepatology | Chronic disease management, specialty pharmacy | Ongoing care coordination |
Specialty practices benefit from medical coding services that understand the nuances of their specific documentation requirements and payer policies. This expertise ensures that complex cases receive appropriate reimbursement.
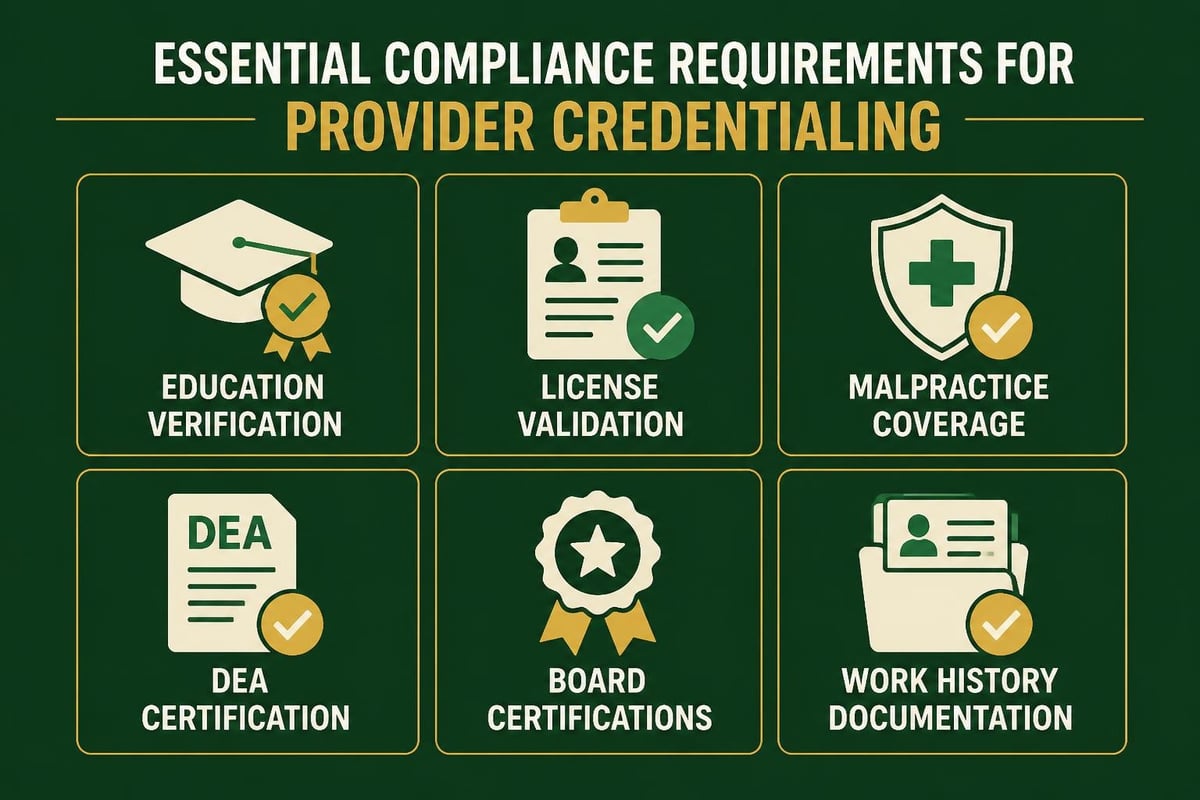
Compliance and Risk Management Integration
Medical management programs must incorporate robust compliance measures to protect both patients and practice financial health. HIPAA compliance, documentation standards, and payer policies create a complex regulatory environment that requires constant attention.
Critical compliance areas include:
- Privacy and security protocols for patient information
- Fraud and abuse prevention measures
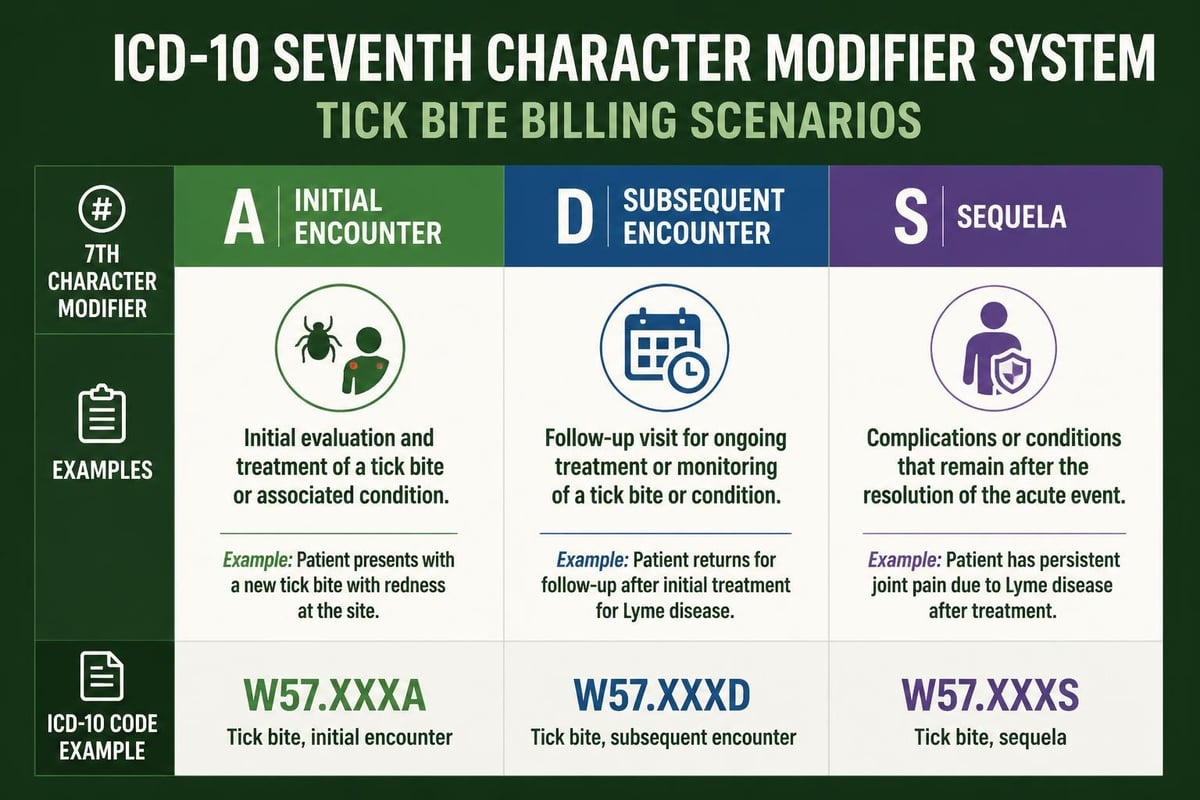
- Proper use of modifiers and coding accuracy
- Medical necessity documentation standards
- Timely filing and claim submission requirements
Understanding contractual adjustments in medical billing helps practices navigate the financial implications of payer agreements while maintaining compliant billing practices. These adjustments represent the difference between billed charges and allowed amounts under contract terms.
Staff Education and Ongoing Training
Successful medical management requires well-trained staff who understand both clinical protocols and administrative requirements. Regular education ensures that team members stay current with evolving guidelines, payer policies, and regulatory changes.
Cross-functional training strengthens the connection between clinical and revenue cycle staff, fostering collaboration that benefits the entire organization. When clinical teams understand billing implications and billing staff grasp clinical rationale, the entire practice operates more efficiently.
Investment in professional development pays dividends through improved accuracy, reduced rework, and enhanced patient satisfaction. Staff who feel competent and confident in their roles deliver better results across all performance dimensions.
Medical management represents the intersection of clinical excellence and operational efficiency, creating sustainable healthcare delivery models that benefit patients and providers alike. By implementing structured protocols, measuring quality outcomes, and maintaining robust documentation practices, healthcare organizations can optimize both care delivery and financial performance. Greenhive Billing Solutions supports these efforts through comprehensive revenue cycle management services that align with clinical operations, ensuring maximum reimbursement while maintaining compliance standards. Our experienced team works within your existing systems to streamline processes, reduce denials, and improve cash flow, allowing your clinical staff to focus on delivering exceptional patient care.